
 Apologies for the length of this post.
Apologies for the length of this post.
As I do every year, I am providing a link on this blog to the annual Scottish stroke care audit – now called the Scottish Stroke Improvement Programme or SSIP as we shall learn to call it in the densely populated world of NHS acronyms.
Those followers of this blog with long memories will quickly realise that the cover (illustrated) has changed little from last year. The same smiling therapist and the same smiling patient are there. I wonder if the patient has progressed significantly since last year; I wonder if the therapist is now a member of a fully integrated multi-disciplinary team helping to provide continued rehabilitation for stroke survivors after they have left acute care. I wonder. I wonder. At least they are both still smiling. Only the date has changed – 2017 has moved inexorably on, as it does, to 2018.
So, has the content changed? Yes, the layout has changed, once again, but maybe not the underlying message, which is – acute stroke care: probably improving slowly, though not all good, and regressing in places; stroke rehabilitation – measured patchily and wildly different across the country.
There is an introduction from the Chief Medical Officer for Scotland, Dr Catherine Calderwood, a woman for whom I have the highest regard, mainly because she has articulated elsewhere a clear vision for health care. Dr Calderwood, as you would expect, uses the word “improvement” on a significant number of occasions throughout her introductory letter, whose message is largely directed towards clinicians and other healthcare professionals.
She quotes evidenced improvements:
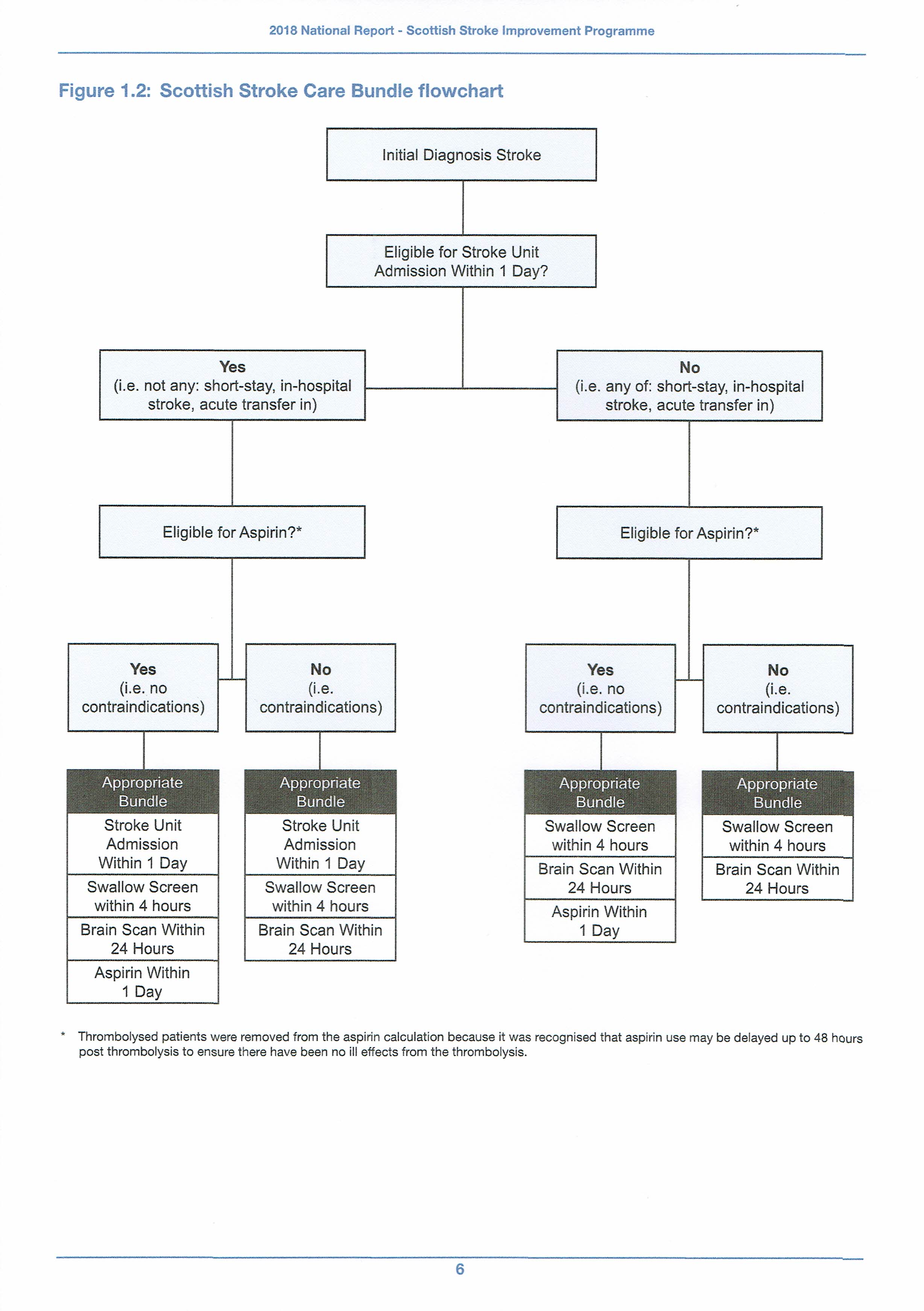
“…….64% patients admitted to hospital with diagnosis of stroke receiving the appropriate elements for the bundle*, a 3% increase on last year.”
The target is 80%. You decide how significant an improvement that is, bearing in mind there are real people at the sharp end of this statistic. Would such a record in terms of punctuality be acceptable on our rail network, for example?
Below is a diagrammatic representation of the “bundle”:
 She mentions desirable improvements relating to outcomes and quality measurements for rehabilitation with which I, along with many stroke survivors, will readily identify. Rehabilitation is a key part of the “patient journey” (horrible phrase) after leaving acute care. Most patients want to resume some sort of quality of life post-stroke, many are realistically capable of achieving this and many younger survivors desire with all their hearts to do so:
She mentions desirable improvements relating to outcomes and quality measurements for rehabilitation with which I, along with many stroke survivors, will readily identify. Rehabilitation is a key part of the “patient journey” (horrible phrase) after leaving acute care. Most patients want to resume some sort of quality of life post-stroke, many are realistically capable of achieving this and many younger survivors desire with all their hearts to do so:
“I encourage Health Boards to provide this information for continued improvements in personalised approach to rehabilitation going forward.”
This tortured sentence is challenging to understand and includes “going forward”, that ugly 21st century phrase suggesting an optimistic but vague future towards which we are all moving and in which everything will be brighter and better. That is not quite the picture of stroke rehabilitation that the SSIP paints. More of this later.
There is an important reference in her introduction to the fact that such improvements as are described in the report are thanks to a wide range of dedicated people:
“These improvements and developments only happen because of the dedication and passion of a large number of people, from frontline staff and carers to co-ordinators and analysts, sometimes in challenging circumstances.”
Having been privileged to see some of these people at work, I’d be tempted to replace the word “sometimes” with “almost always”.
Finally, Dr Calderwood references her own impressive past papers on Realistic Medicine:
“Reducing unwarranted variation is a priority in Realistic Medicine and I encourage you to use the quality audit data and the improvement programme to seek ways to make progress towards the standards of care.”
“Progress towards the standards of care” – an acknowledgement that we are not yet reaching the standards we aspire to. This failure is much evidenced in the report. And what about “unwarranted variation” – an Orwellian understatement and the hallmark of post-acute stroke care across Scotland. In simple human terms, if you leave hospital alive after a stroke, the care you will get is a healthcare lottery depending on where you happen to live.
I have spent a lot of this post describing Dr Calderwood’s introductory letter, for which I make no apology as it sums up some key points in the audit. Her underlying message, while trying not to discourage the troops, is that things must improve. They must.
As for the details of the data, I can do no better than quote a section of the response to the audit from the Director of the Stroke Association in Scotland:
We are pleased to note the improvements outlined in the audit, but some serious challenges remain.
Most notably, we are disappointed to see a significant number of hospitals not performing well against the standard set for delivering thrombolysis**. The earlier a clot is dissolved with thrombolysis which unblocks an artery and allows blood to flow through the brain, the less disability will be experienced.
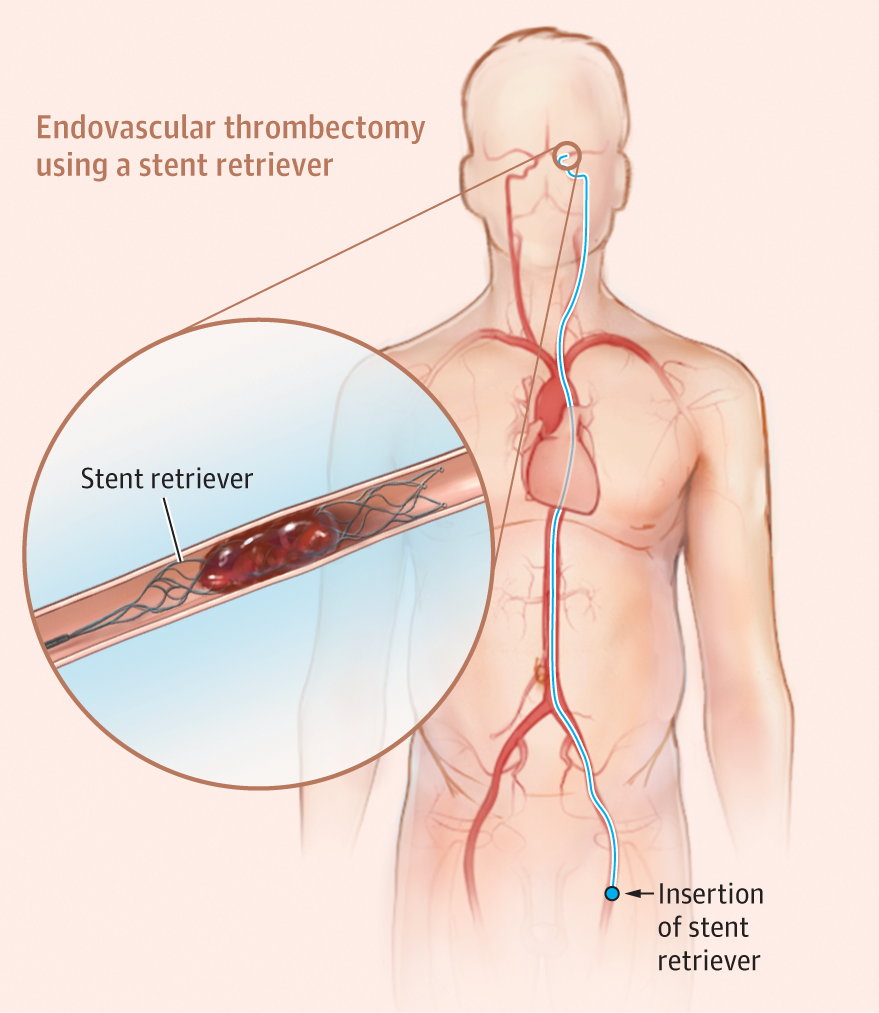
We are also extremely concerned about the delivery of thrombectomy***.
In 2017, only 13 people received thrombectomy, and currently no centre in Scotland is providing it. The Audit identifies around 600 Scots per year as potentially benefiting from this life changing treatment. A national committee has been established to plan a Scottish thrombectomy service, but the process is slow and the consequence again is that many patients have been left with worse outcomes and significant disability.
We are calling alongside Chest, Heart and Stroke Scotland for the provision of thrombectomy in Scotland to be tackled as a priority by the Scottish Government, with national funding identified by the NHS. Those eligible stroke patients in Scotland deserve the same access to this life-changing treatment as in England.
For me, this is the heart of the matter – at the strategic centre of stroke care planning in Scotland, we need ambition and vision. We seem to lack this at the moment. All the statistics we have show that, in terms of care for stroke, Scotland is falling behind many countries in the developed world, let alone our nearest neighbours in England. Page 9 of the audit is particularly blunt in this regard:
In the developed world many areas have developed Comprehensive Stroke Centres (centres that deliver all aspects of stroke care, including stroke thrombectomy). Currently there are no Comprehensive Stroke Centres in Scotland.
 Stroke is a medical emergency demanding as much urgency as, say, a heart attack. The type of stroke must be quickly ascertained and the correct subsequent procedures followed. As the report admits, hundreds of people who survive a stroke could have had a better quality of life (note the verb tense – “could have had”). In other words they could have had less disability, could have had less demands on their families, could have had less need of expensive personal care and overall could have had a better quality of life if thrombolysis targets had been met and thrombectomy had been available, for those for whom it was suitable. They are the lost opportunities – the could have hads – a silent shambling army, with damaged brains and weakened bodies, but wistful thoughts of what might have been.
Stroke is a medical emergency demanding as much urgency as, say, a heart attack. The type of stroke must be quickly ascertained and the correct subsequent procedures followed. As the report admits, hundreds of people who survive a stroke could have had a better quality of life (note the verb tense – “could have had”). In other words they could have had less disability, could have had less demands on their families, could have had less need of expensive personal care and overall could have had a better quality of life if thrombolysis targets had been met and thrombectomy had been available, for those for whom it was suitable. They are the lost opportunities – the could have hads – a silent shambling army, with damaged brains and weakened bodies, but wistful thoughts of what might have been.
Nothing worthwhile is ever achieved easily, as any stroke survivor will tell you. I may be howling at the moon, but I urge Jeane Freeman, our new Cabinet Secretary for Health, not just to make stroke care a priority, but to make Scotland a world leader in stroke care. That would be a great legacy for her, but, more importantly, it is no less than stroke survivors and their families deserve.
______________________________________________________________________________________________
* bundle – a prescribed set of procedures which must take place as soon as possible following all stroke diagnoses
** thrombolysis – an injection which must be given within four hours to dissolve a blood clot in the brain
***thrombectomy – a skilled procedure to remove a blood clot mechanically from the brain. Can hugely improve outcomes for certain patients